
Part III: Dr. Judah Folkman — Would He Be Funded Today?

In Part II, I asked you to hold one number in your head: 33 years.
That’s how long Folkman’s idea took to travel from a hypothesis his peers called the work of a “clown” to bevacizumab’s FDA approval in 2004. Three decades of failed grants, emptied conference rooms, near-resignation, and a seven-year cycle of hype and collapse — and at the end of it, a permanent pillar of cancer medicine.
Now run the experiment forward. Suppose a young surgeon walked into an NIH study section today with the 1971 idea: against consensus, from the wrong specialty, promising drugs decades away. Would the system we’ve built in 2025 and 2026 give that person the same long runway that Folkman barely got?
I don’t think the answer is obviously yes. And the reason isn’t a single villain or a single budget line. It’s the texture of how research is being funded right now.
What actually happened to the money
Let me be careful here, because the real story is alarming enough without exaggeration — and the nuance is the whole point.
The stated ambition was dramatic. The administration’s FY2026 budget sought to cut NIH from roughly $48 billion to about $27.5 billion — nearly 40% — and to collapse the agency’s 27 institutes and centers into eight. The National Cancer Institute was slated for a roughly 37% cut.
Congress, to its credit, rejected the headline cut. The bipartisan deal reached in early 2026 set NIH at about $48.7 billion — a slight increase — and included language meant to block the gutting of the “indirect cost” payments that keep labs running. If you only read the topline number, you’d think the crisis was averted.
It wasn’t. The damage was inflicted through a hundred smaller administrative actions that didn’t require Congress’s permission — an indirect-cost cap, mass grant terminations, trials stopped mid-stream, and a peer-review system that seized up. Here’s the year in numbers:
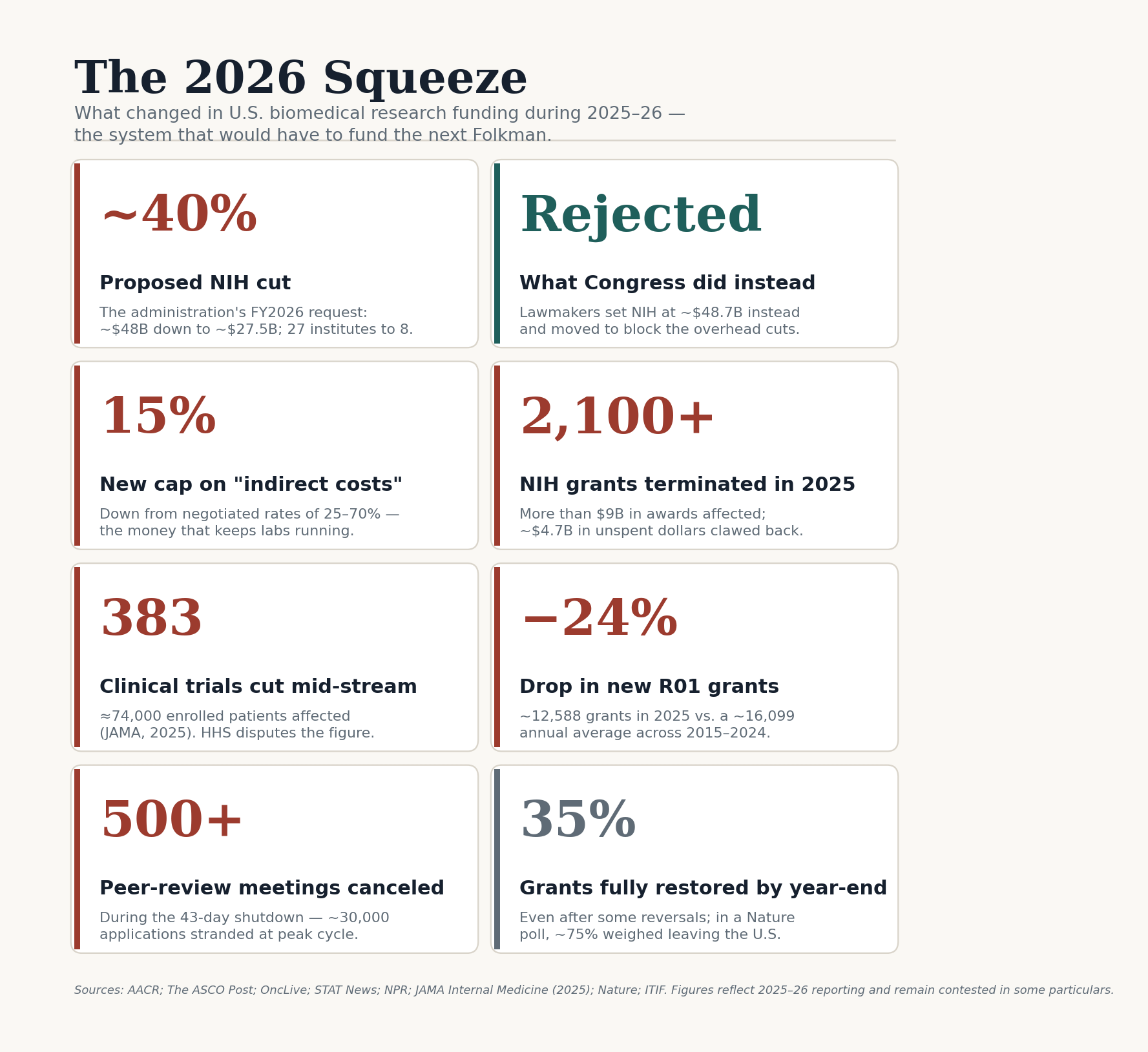
Each of those cards tells its own story. The 15% cap on indirect costs, down from negotiated rates of 25–70%, isn’t an attack on bureaucracy — it’s a cut to the money that keeps freezers cold and lab doors open. The 2,100-plus terminated grants clawed back billions in research dollars, already partially spent. And the 383 clinical trials cut mid-stream left roughly 74,000 enrolled patients in limbo — some losing access to an active treatment — though HHS publicly disputes that figure and, as of early 2026, had not produced the grant-by-grant accounting lawmakers requested to support its much smaller number.
The quiet part: peer review itself broke down
Money is the visible story. The harder-to-see story is what happened to the judgment system — and that’s the part most relevant to a Folkman.
NIH’s gold standard is peer review by “study sections”: standing panels of working scientists who weigh proposals on scientific merit. In 2025, that machinery seized up. Winter panels were canceled and rescheduled in confusion. An advisory council that guided fair-review practices was abruptly disbanded. Review was forcibly centralized. Then the 43-day government shutdown beginning October 1 forced NIH to cancel more than 500 review meetings, stranding the review of roughly 30,000 applications at the peak of the fall cycle. Researchers reported that grants submitted in mid-2025 were not looked at until early 2026. On top of the delays, NIH announced it would stop treating peer-review scores as strict funding cutoffs — folding in “other factors” and instituting priorities, which many scientists read as opening the door to political rather than scientific selection.
Here’s why that’s the dangerous part, and why I keep coming back to Folkman specifically.
A radical, against-consensus proposal is exactly the kind that dies first when review is rushed, understaffed, centralized, and steered by “priorities” and immediate payback. Folkman’s 1971 idea was, by the standards of its day, a high-risk bet from someone outside the relevant specialty, contradicting settled dogma and promising drugs decades out. That is precisely the profile a stressed, ROI-focused system sheds. You don’t have to reject a Folkman on purpose. You just have to make the system impatient, and it discards the long shots on its own.
Two questions everyone asks
“How long to get back to baseline?” Longer than the budget cycle that caused the damage. The thing being damaged isn’t a line item; it’s an ecosystem — labs, mentors, equipment, trainees, institutional memory. When a lab loses 40% of its people, publication output can fall by ~90%. Even after some terminations were reversed and the topline budget restored, only about a third of researchers whose grants were cut or delayed reported full restoration by year’s end. Surveys show roughly three-quarters of U.S. scientists are considering moving abroad, and other countries are actively recruiting them. Rebuilding lost capacity takes years, possibly a decade — and in some specialties, talent that leaves may not return. A research workforce is not a faucet you can shut off and turn on again.
“How long to get back to baseline?” Longer than the budget cycle that caused it. The thing being damaged isn’t a line item; it’s an ecosystem — labs, mentors, equipment, trainees, institutional memory. When a lab loses 40% of its people, publication output can fall by ~90%. Even after some terminations were reversed and the topline budget restored, only about a third of researchers whose grants were cut or delayed reported full restoration by year’s end. Surveys show roughly three-quarters of U.S. scientists are considering moving abroad, and other countries are actively recruiting them. Rebuilding lost capacity is measured in years, plausibly a decade, and in some specialties, talent that leaves may simply not come back. A research workforce is not a faucet you can shut off and turn on again.
The question this leaves us with…
We’ve established the machine: impatient, understaffed, tilted toward immediate payback, and missing some of the people who would have run it. A 2026 Folkman might still get in the door — but the door is narrower, and it closes faster on exactly his kind of idea.
Which raises the question I want to sit with in the final part of this series. We’ve spent three parts establishing how close the angiogenesis story came to not happening, and how much harder it would be to reproduce its conditions today. So let’s make the stakes concrete. If that idea had been filtered out — if a younger Folkman had simply moved on when the grants dried up — what exactly would be missing from medicine right now?
Read More: Part IV: A World Without Folkman»
I have authored and edited this article. AI has been used to assist with background research and formatting. Sources include reporting and analysis from The ASCO Post, OncLive, STAT News, NPR, JAMA Internal Medicine, JAMA Health Forum, the AACR, the American Cancer Society Cancer Action Network, the Information Technology and Innovation Foundation, and Nature. Figures on the 2025–26 cuts reflect the best available reporting as of mid-2026 and remain contested in some particulars, notably between independent researchers and HHS.