
The Dr. Judah Folkman Test
What a “heretic” surgeon’s 30-year fight against cancer reveals about the research system we’re dismantling, and asks "Would his pioneering cancer research be funded today?"

I vividly recall reading the front-page New York Times article, “A Cautious Awe Greets Drugs That Eradicate Tumors in Mice" (May 3rd, 1998). I was having lunch and reading the newspaper in St. Catherine’s Park, across from Memorial Sloan-Kettering Cancer Center, where I was completing my research fellowship in psychosocial oncology. The headline immediately grabbed my attention. The article explained how Dr. Judah Folkman and his Harvard lab had identified a molecule in mouse urine that prevents the formation of new blood vessels, which normally supply tumors with nutrients needed for growth. I remember sitting there, reading carefully, occasionally looking up at the sky and laughing, murmuring, “Mouse urine. Really? Wow. Now that’s just wild.” Although ostracized by the oncology community early on, Dr. Folkman coined the term “antiangiogenesis,” and this groundbreaking discovery has transformed current approaches to treating cancer and other diseases. I will never forget reading that article, as it broadened my perspective and made me realize that even when faced with obstacles, the seemingly impossible can sometimes be achieved.
Today, we are living through a strange contradiction. On one screen, the headlines promise a golden age: AI platforms that fold proteins, design molecules, and read tumors with a fluency that would have seemed like science fiction a decade ago—tools genuinely poised to reshape how we treat both novel and long-standing diseases. On the other screen, the machinery that turns wild ideas into actual medicines is being starved. Over the course of 2025 and into 2026, the federal government cut billions from biomedical research, capped the funds that keep university labs running, terminated thousands of grants, and let a 43-day shutdown freeze the entire grant-review system.
It raises an uncomfortable question, and it’s worth asking plainly:
In a research climate that prizes immediate, demonstrable return on investment and dismisses high-risk, “fringe” theories as a waste of money, would Judah Folkman—the surgeon who founded an entire field of cancer medicine—ever have gotten his shot?
Folkman is the cleanest possible test case, because for the better part of three decades, almost everyone thought he was wrong. This is a story about how transformative medicine actually gets made, and about what we stand to lose when we forget.
Part One — The Heretic Who Was Right
A surgeon notices something nobody else will explain
In the 1960s, Judah Folkman was not supposed to be a theorist. He was a prodigy surgeon—into Harvard Medical School at 19, surgeon-in-chief at Boston Children’s Hospital, and a full professor of surgery by his mid-thirties. But while perfusing isolated organs during his Navy research years, he kept noticing the same thing: tumors implanted without a blood supply simply stopped growing. They’d reach the size of a pinhead and stall, dormant, unable to expand past a millimeter or two.
In 1971, he put the idea in print in The New England Journal of Medicine. The hypothesis was radical and tidy:
Tumors can’t grow beyond a tiny size without recruiting new blood vessels.
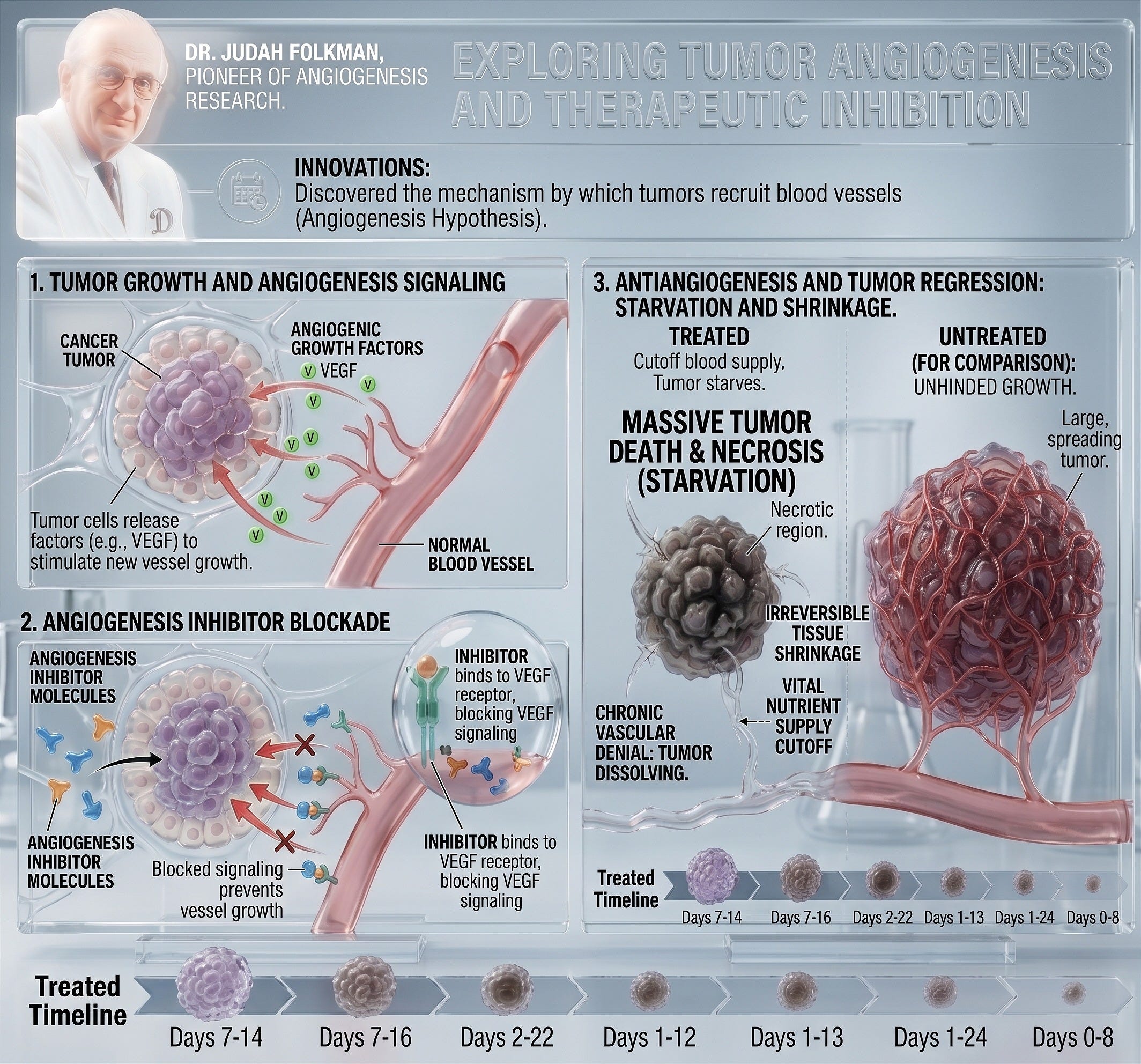
Tumors can’t build those vessels themselves, so they must send chemical signals that trick the body into building the vessels for them—a process called angiogenesis.
Therefore, a drug that blocks angiogenesis could starve a tumor and hold it in check.
He even coined the term for the strategy—antiangiogenesis—and predicted that someone would eventually identify the tumor’s secreted “angiogenic factor” and build a drug against it. He was describing medicines in 1971 that wouldn’t exist until 2004.
“Heresy,” and the years in the wilderness
The response was not polite skepticism. It was ridicule. The prevailing dogma held that the new vessels around a tumor were just inflammation—the body’s reaction to dying cells—not a precondition that the tumor actively required. Folkman’s paper was treated as heresy. Reviewers complained his conclusions ran far ahead of his data. Colleagues openly questioned whether a surgeon had any business making molecular claims at all. One former student later described it as Folkman fighting “the tunnel vision of that time.”
This is the part of the story that matters most for our question, so it’s worth being precise about it: the skepticism didn’t just bruise his ego—it hit his funding. His difficulty persuading peers translated directly into difficulty getting NIH grants, difficulty publishing, and difficulty recruiting young scientists willing to bet their careers on a theory the establishment had written off. For years, he ran a lab around an idea most study sections considered, at best, speculative and unfundable.
He kept going anyway—famously resolving to pursue the hypothesis alone if he had to, until he either proved or disproved it. That stubbornness is usually told as an inspirational character note. Read it instead as a warning: the system worked despite itself, and only because Folkman had the seniority, the surgical income, the institutional perch, and the sheer obstinacy to outlast a decade-plus of rejection. Strip any one of those away, and the field never gets founded.
The proof, and the fellows who built it
Vindication came in stages, largely through the people Folkman trained. His lab became a factory for the evidence the field needed:
Donald Ingber helped identify the fungal compound fumagillin as an angiogenesis inhibitor.
Robert D’Amato discovered in 1994 that thalidomide—the infamous drug that had caused birth defects decades earlier—worked by blocking angiogenesis. That insight led directly to thalidomide and its analogs becoming real treatments for multiple myeloma, a blood cancer.
Michael O’Reilly isolated the body’s own angiogenesis inhibitors—angiostatin in 1994 and endostatin in 1997—which in mice could regress tumors and hold them dormant.
The endostatin results, in particular, triggered a frenzy. The above-referenced 1998 New York Times front-page story quoting a Nobel laureate’s offhand enthusiasm set off public expectations that Folkman was about to “cure cancer in two years.” He hadn’t promised that, and the mouse results didn’t translate cleanly to humans—an early, painful lesson that the field’s hype could outrun its biology.
The real clinical breakthrough came from outside his lab, but straight out of his theory. At Genentech, Napoleone Ferrara identified vascular endothelial growth factor (VEGF) in 1989—the diffusible signal Folkman had predicted 18 years earlier—and the company built an antibody to block it. In 2004, the FDA approved that drug, bevacizumab (Avastin), for metastatic colorectal cancer. It was the first antiangiogenic cancer drug, arriving 33 years after the NEJM paper that got Folkman branded a crank. He died in 2008, by which point about a dozen angiogenesis-targeting drugs were on the market.
What antiangiogenesis actually delivered—the honest version
Here it’s tempting to reach for a triumphant “lives saved” number, and you’ll see big ones cited. I’d urge caution with those metrics, as the honest picture is more interesting than the marketing one.
The footprint is genuinely enormous. Bevacizumab went on to be approved across colorectal, lung, kidney, cervical, ovarian, and brain cancers, and has been given to millions of patients worldwide. A whole class followed it—drugs like sorafenib, sunitinib, pazopanib, aflibercept, ramucirumab, and others—plus, in a beautiful piece of biological irony, the same VEGF-blocking approach revolutionized the treatment of wet macular degeneration, saving the sight of enormous numbers of older adults. An entire industry now rests on a hypothesis once dismissed as heresy.
But the survival math is genuinely debated, and a credible piece should say so. For many solid tumors, antiangiogenic drugs reliably slow disease progression yet produce modest—or sometimes no—gains in overall survival, often at real cost and toxicity. Bevacizumab’s strongest survival case remains metastatic colorectal cancer; its breast cancer approval was actually withdrawn by the FDA in 2010 when follow-up trials failed to show a survival benefit worth the risks. So the truthful claim isn’t “antiangiogenesis cured cancer.” It’s something subtler and, for our purposes, more important: a hypothesis everyone hated turned out to be a fundamental, durable pillar of how we now understand and treat cancer—one of the recognized hallmarks of the disease, a permanent target class, and the seed of treatments now woven through oncology and other fields alike.
That payoff took more than thirty years to mature. Hold that number in your head for Part Two…
I have authored and edited this article. AI has been used to assist with background research and formatting. Sources include reporting and analysis from The ASCO Post, OncLive, STAT News, NPR, JAMA Internal Medicine, JAMA Health Forum, the AACR, the American Cancer Society Cancer Action Network, the Information Technology and Innovation Foundation, Nature, and the PNAS and Cell retrospectives on Folkman's career. Figures on the 2025–26 cuts reflect the best available reporting as of mid-2026 and remain contested in some particulars, notably between independent researchers and HHS.